
Diagnostic performance and operational feasibility of the VISITECT CD4 lateral flow assay for advanced HIV disease in Kenyan public health facilities: a cross-sectional study
John Mungai Kuria, Tom Marwa Machera, Kathryn Nderitu
Corresponding author: John Mungai Kuria, School of Public Health, Amref International University, Nairobi, Kenya 
Received: 11 May 2026 - Accepted: 17 Jun 2026 - Published: 02 Jul 2026
Domain: Clinical laboratory sciences
Keywords: Feasibility studies, HIV infections, Kenya, predictive value of tests, point-of-care testing, diagnostic tests
Funding: This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
©John Mungai Kuria et al. Primary Health Care Practice Journal (ISSN: 3105-7624). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: John Mungai Kuria et al. Diagnostic performance and operational feasibility of the VISITECT CD4 lateral flow assay for advanced HIV disease in Kenyan public health facilities: a cross-sectional study. Primary Health Care Practice Journal. 2026;5:3. [doi: 10.11604/PHCP.2026.5.3.53296]
Available online at: https://www.phcp-journal.org//content/article/5/3/full
Research 

Diagnostic performance and operational feasibility of the VISITECT CD4 lateral flow assay for advanced HIV disease in Kenyan public health facilities: a cross-sectional study
Diagnostic performance and operational feasibility of the VISITECT CD4 lateral flow assay for advanced HIV disease in Kenyan public health facilities: a cross-sectional study
John Mungai Kuria1,&, ![]() Tom Marwa Machera1,
Tom Marwa Machera1, ![]() Kathryn Nderitu2
Kathryn Nderitu2
&Corresponding author
Introduction: advanced HIV disease (AHD), defined as CD4 below 200 cells/mm3 or World Health Organization (WHO) clinical stage III/IV, drives the majority of HIV-related early mortality. Kenya's conventional CD4 infrastructure is centralized, achieving only 20.1% testing coverage among eligible persons. The VISITECT CD4 lateral flow assay (LFA) offers 40-minute point-of-care results without laboratory infrastructure. Kenya-specific diagnostic performance data under routine programme conditions were absent prior to this study.
Methods: a cross-sectional study was conducted from December 2025 to April 2026 across four public health facilities in Homa Bay, Nairobi, and Kiambu counties (n=326 people living with HIV (PLHIV)). VISITECT LFA was performed in parallel with conventional CD4 (Alere PIMA at Homa Bay CTRH and Thika Level 5; CyFlow Partec at Kenyatta National Hospital (KNH) and Mama Lucy Kibaki Hospital). Two independent VISITECT reads were performed per participant: read 1 by a laboratory technologist and read 2 by a clinician blinded to both read 1 and the conventional result. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, and Cohen's kappa were calculated; binary logistic regression identified independent AHD predictors.
Results: overall AHD prevalence was 39.3% (128/326). VISITECT read 1 achieved a sensitivity of 99.2% (95%CI 95.7-99.9%), specificity 89.9% (84.9-93.4%), NPV 99.4%, PPV 86.4%, accuracy 93.6%, and kappa 0.868. Read 2 (clinician) achieved a sensitivity of 96.1%, specificity 87.9%, and kappa 0.818. Inter-reader agreement was near-perfect (kappa=0.938, 96.9% concordance). All 128 AHD cases occurred exclusively among virally unsuppressed participants (prevalence 62.1% vs 0%). AHD was independently predicted by Kiambu County (aOR 4.63), male sex (aOR 2.40), and interruption in treatment (IIT) returnee status (aOR 1.88).
Conclusion: VISITECT CD4 LFA demonstrates near-perfect sensitivity and cross-cadre reproducibility in Kenyan public facilities. The complete separation of AHD by viral load status and the higher-than-expected AHD burden (39.3%) provide the National AIDS and STIs Control Program (NASCOP) with evidence to prioritise rollout at facilities serving virally unsuppressed patients and to integrate VISITECT into differentiated AHD screening algorithms.

Advanced HIV Disease (AHD), defined as CD4 below 200 cells/mm3 or WHO clinical stage III/IV, accounts for over 50% of AIDS-related mortality globally and drives early mortality rates of 15-25% within three months of antiretroviral therapy (ART) initiation [1-3]. The WHO-AHD package of care, incorporating TB-LAM testing, cryptococcal antigen screening, and opportunistic infection prophylaxis, can reduce this mortality burden by 35-40% when initiated at treatment start, but requires timely CD4 count to trigger its deployment [4].
In Kenya, 32.5% of HIV-infected individuals who are not yet virally suppressed - and are therefore eligible for CD4 testing under national guidelines - have AHD as defined by CD4 <200 cells/mm3, yet only 20.1% received CD4 testing in the mid-2024 national reporting period [5-7]. The root cause is infrastructure: Kenya's conventional CD4 platforms, the Partec CyFlow at county and referral hospitals and the Alere PIMA at secondary facilities, require electricity, laboratory-grade environments, cold-chain reagent storage, and trained operators, producing result turnaround times of two to seven days that prevent same-visit clinical action [8-10]. In rural high-burden counties such as Homa Bay (HIV prevalence 17%), Siaya (~19.3%), and Kisumu (~17.5%) (KENPHIA 2018/NASCOP 2022 data), where laboratory infrastructure is sparse and patient volumes are high, this turnaround delay translates directly into missed AHD diagnoses and preventable mortality.
The VISITECT CD4 Advanced Disease Test (AccuBio Biotech Co. Ltd.) is a WHO-prequalified (PQDx 0238) semi-quantitative lateral flow immunoassay that identifies CD4 at or below 200 cells/mm3 using finger-prick whole blood, with results in 40 minutes and no electricity, cold chain above 30°C, or laboratory infrastructure requirement [11]. Published multi-country evaluations report sensitivity ranging from 91.3% to 96.4% and specificity from 91.3% to 97.1%: Ndlovu et al. (2020) in Zimbabwe (sensitivity 91.3%, specificity 96.6%) [9]; Haraka et al. (2024) in Tanzania (sensitivity 96.4%, specificity 95.1%) [10]; Gils et al. (2024) across seven countries (pooled sensitivity 94.8%, specificity 94.3%, n>3,000) [12]; and Lechiile et al. (2022) under controlled laboratory conditions (kappa 0.88) [13]. These studies established the diagnostic validity of VISITECT but were conducted in heterogeneous settings and under varying operational conditions. The VISITECT CD4 advanced disease test was also evaluated in Kenya by the Kenya Medical and Research Institute (KEMRI) in 2022, as documented in the WHO public report on VISITECT CD4, confirming acceptable diagnostic performance under controlled conditions prior to this routine-programme evaluation (KEMRI/WHO, 2022).
A critical gap in the evidence base was the absence of Kenya-specific diagnostic performance data under routine programme conditions. Critically, no prior study had simultaneously assessed diagnostic performance by two different healthcare cadres, laboratory technologists and clinicians, to evaluate inter-reader agreement and the validity of cross-cadre task-shifting. This distinction matters for Kenya's implementation plan: if clinicians can reliably interpret VISITECT results without specialist laboratory training, the test can be deployed by the larger clinical officer and nursing workforce that staffs the majority of Kenya's HIV clinics, dramatically extending diagnostic reach. This study was designed to provide both the performance data and the inter-reader reproducibility evidence that NASCOP required for deployment policy development.

Study design: we conducted a cross-sectional diagnostic accuracy and feasibility study of point-of-care semi-quantitative CD4 testing using the VISITECT CD4 advanced disease test, with concurrent reference-standard laboratory CD4 enumeration, integrated into routine HIV testing services. The study is reported in accordance with the strengthening the reporting of observational studies in epidemiology (STROBE) statement for cross-sectional studies.
Setting: the study was conducted at four public health facilities representing a range of levels in Kenya's tiered healthcare system: Kenyatta National Hospital (KNH), a level 6 national referral hospital in Nairobi County; Homa Bay County Referral Hospital (HBCTRH), a level 5 county referral hospital in Homa Bay County; Thika Level 5 Hospital, a level 5 sub-county hospital in Kiambu County; and Mama Lucy Kibaki Hospital, a level 4 county hospital in Nairobi County. These facilities collectively serve diverse patient populations in high-burden urban, peri-urban, and high-HIV-prevalence lake-region settings, in accordance with the ministry of health programmatic guidelines for advanced HIV disease management [14]. Sites were selected to represent the range of operational environments in which a point-of-care CD4 assay would be deployed at scale, from tertiary national referral to primary county hospitals.
Participants: eligible participants were adults (≥18 years) presenting to participating sites for HIV testing or treatment services who were able to provide written informed consent. Inclusion criteria were confirmed HIV-positive status (either newly diagnosed or established on treatment as defined by the protocol) and willingness to provide a finger-prick blood sample for the index test and a venous sample for the reference standard. The sole formal exclusion criterion was a contraindication to venipuncture. Enrolled participants included HIV-positive individuals presenting for routine testing or clinical review, irrespective of whether a CD4 test was indicated at that visit under standard protocols; all consenting eligible individuals were offered VISITECT testing alongside the flow cytometry reference standard. Consecutive eligible participants were enrolled to minimize selection bias.
Variables: the primary outcome was the diagnostic accuracy of the VISITECT CD4 advanced disease test (index test) for identifying CD4 ≤200 cells/mm3 relative to flow cytometric CD4 enumeration (reference standard). Secondary outcomes were operational feasibility indicators (time to result, proportion of valid results, user-reported usability) and patient acceptance rate (proportion of eligible individuals consenting to VISITECT testing when offered during routine service delivery). Participant-level covariates included age, sex, antiretroviral therapy (ART) status (naïve vs. experienced), and clinical presentation.
Data sources/measurement: the index test was performed at the point of care by trained healthcare workers on a finger-prick whole-blood sample, in accordance with the manufacturer's instructions, with results read visually at 40 minutes and recorded as CD4 ≤200 or >200 cells/mm3. The reference test was a venous ethylenediaminetetraacetic acid (EDTA) sample analyzed by flow cytometry at the nearest accredited laboratory using standard operating procedures. Index- and reference-test results were recorded on standardized case report forms and double-entered into a study database. Operators performing the index test were blinded to the reference result, and laboratory technicians performing the reference test were blinded to the index result.
Bias: to limit selection bias, we enrolled consecutive eligible participants at each site. To limit information bias, index- and reference-test results were read and recorded independently and blinded as described above. To limit verification bias, the reference standard was performed on all enrolled participants regardless of the index-test result. We pre-specified the analysis plan to limit selective reporting.
Study size: the target sample size was calculated to estimate the sensitivity of the index test at CD4 ≤200 cells/mm3 with adequate precision (95% confidence interval half-width ≤5%), assuming an expected sensitivity of 0.94 based on prior multi-country evaluations [9,10,12,13] and an anticipated prevalence of CD4 ≤200 cells/mm3 among enrolled participants consistent with national surveillance estimates [5]. The sample size was inflated by 10% to account for an anticipated proportion of invalid or missing results, yielding a target enrolment of 355.
Quantitative variables: CD4 cell count from the reference standard was analyzed both as a continuous variable (cells/mm3) and as a binary variable (≤200 vs. >200 cells/mm3) corresponding to the threshold used by the index test. Age was analyzed continuously and in pre-specified categories (18-24, 25-34, 35-49, ≥50 years). Time-to-result was not systematically logged for each participant; however, all tests were performed within the manufacturer-specified 40-minute reading window.
Statistical methods: diagnostic accuracy was summarized as sensitivity, specificity, positive and negative predictive values, and the corresponding 95% confidence intervals (Wilson score interval) using the reference standard as the gold standard. Agreement between index and reference results was quantified using Cohen's kappa. Feasibility outcomes were summarized using proportions for categorical variables and medians with interquartile ranges for continuous variables. Subgroup analyses pre-specified by sex, age group, and ART status were performed. Missing data were reported transparently and analyzed under a complete-case approach, with sensitivity analyses examining the impact of plausible patterns of missingness. All analyses were performed in SPSS version 27.0 (IBM Corp., Armonk, NY) and Excel. Statistical significance was set at p<0.05.
Ethical considerations: the study was conducted in accordance with the Declaration of Helsinki. Ethical approval was granted by the Amref Health Africa Ethics and Scientific Review Committee (Amref ESRC) under reference number P2005/2025, and research authorization was obtained from the National Commission for Science, Technology and Innovation (NACOSTI) under reference NACOSTI/P/26/4183389, with additional approvals from the county directors of health in Homa Bay, Nairobi, and Kiambu counties. Written informed consent was obtained from all adult participants prior to enrolment, with consent forms available in English and Kiswahili. Healthcare workers performing VISITECT result reading were provided with a written participant information sheet and provided written informed consent prior to any study activity. The study protocol required all reference standard CD4 results to be disclosed to the managing clinician on the same visit; participants found to have CD4 <200 cells/mm3 by the reference method were linked to the NASCOP Advanced HIV disease package of care (TB-LAM, cryptococcal antigen screening, cotrimoxazole prophylaxis, and enhanced clinical monitoring) within the same clinical encounter. All data were collected using anonymized study codes and stored in password-protected, access-restricted systems.
Participants and descriptive data: participants were enrolled consecutively from December 2025 to April 2026. A total of 326 persons living with HIV (PLHIV) were enrolled: Homa Bay County Referral Hospital (HBCTRH) (138) (42.3%), Thika Level 5 Hospital (78) (23.9%), Kenyatta National Hospital (KNH) (60) (18.4%), and Mama Lucy Kibaki Hospital (50) (15.3%). Mean age 37.9 years (SD 13.7); 56.4% female. Eligibility categories: newly enrolled 45.7%, virological failure 30.7%, interruption-in-treatment (IIT) returnees 23.6%. Most participants were on a tenofovir/lamivudine/dolutegravir (TLD) regimen (68.7%); 63.2% had unsuppressed viral loads, reflecting the clinical profile of a CD4-testing-eligible population (Table 1). For the purposes of diagnostic accuracy analysis, the binary outcome was CD4 ≤200 cells/mm3 as the clinically actionable threshold operationalized by the VISITECT assay. Overall prevalence of CD4 ≤200 cells/mm3 was 39.3% (128/326), substantially exceeding the 30% assumption in sample size calculations; patients with WHO clinical stage 3 or 4 and CD4 >200 cells/mm3 represent a recognized limitation of this CD4-based AHD prevalence estimate.
Advanced HIV disease (AHD) prevalence differed significantly by county (Kiambu 56.4%, Nairobi 45.5%, Homa Bay 24.6%; chi-square=23.76, p<0.001) and sex (males 47.9% vs females 32.6%; chi-square=7.22, p=0.007). The immunovirological relationship between viral load and CD4 count is well established: uncontrolled HIV replication drives progressive CD4+ T-cell depletion through direct viral cytopathic mechanisms and immune activation; viral suppression is associated with CD4 recovery in the majority of adherent patients. While the directionality of this relationship is expected, the magnitude of separation observed here constitutes a novel and operationally actionable programmatic finding: all 128 cases of CD4 ≤200 cells/mm3 occurred exclusively among the 206 participants with unsuppressed viral loads (CD4 ≤200 cells/mm3 prevalence 62.1%), while zero such cases were found among the 101 participants with suppressed viral loads (chi-square=122.77, p<0.001). Median CD4 was 157 cells/mm3 among unsuppressed vs 488 cells/mm3 among suppressed participants. WHO clinical stage showed no significant association with CD4 counts (p=0.946). In adjusted logistic regression, independent predictors of CD4 ≤200 cells/mm3 were Kiambu County (aOR 4.63, 95%CI 2.47-8.67, p<0.001), Nairobi County (aOR 2.87, 95%CI 1.63-5.05, p<0.001), male sex (aOR 2.40, 95%CI 1.47-3.93, p<0.001), and interruption-in-treatment (IIT) returnee status (aOR 1.88, 95%CI 1.09-3.25, p=0.024) (Table 2).
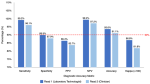
Outcome data and main results: read 1 (laboratory technologist) achieved a sensitivity of 99.2% (95%CI 95.7-99.9%), with a single false negative: a newly enrolled patient at Thika Level 5 with a conventional CD4 of 81 cells/mm3. Twenty false positives had a median conventional CD4 of 248 cells/mm3 (IQR 215-328). Read 2 (clinician) demonstrated slightly lower sensitivity (96.1%) and specificity (87.9%), representing the expected reduction when non-laboratory cadres interpret results. Overall accuracy was 93.6% for read 1 and 91.1% for read 2 (Figure 1).
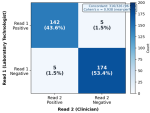
Inter-reader agreement between laboratory technologist and clinician was near-perfect: kappa=0.938 with 316/326 concordant readings (96.9%). Only five discordant results were recorded in each direction (read 1 positive/read 2 negative: n=5; read 1 negative/read 2 positive: n=5). This level of agreement confirms that VISITECT result interpretation is highly reproducible across cadres under routine programme conditions (Figure 2).
Other analyses: facility-level performance ranged from kappa=0.966 at KNH (specificity 97.0%) to kappa=0.763 at Mama Lucy Kibaki Hospital (specificity 77.8%). The lower specificity at Mama Lucy (six false positives from 27 non-AHD participants) was not explained by participant characteristics and suggests an operational or environmental factor requiring site-level investigation. Sensitivity was 100% at three of four facilities (KNH, Homa Bay CTRH, Mama Lucy). By eligibility category, IIT returnees had the highest kappa (0.948) and treatment failure the lowest (0.800), though all three exceeded the 0.80 near-perfect agreement threshold.
This study reports near-perfect VISITECT CD4 LFA sensitivity (99.2%), clinically acceptable specificity (89.9%), near-perfect inter-reader agreement (kappa=0.938), and an AHD prevalence of 39.3%, substantially exceeding national estimates, entirely concentrated among virally unsuppressed participants. These findings collectively provide NASCOP with the operational evidence base to formalize VISITECT deployment and to integrate it into a precision AHD identification strategy targeting virally unsuppressed patients.
The sensitivity of 99.2% observed in this study exceeds the pooled sensitivity of 94.8% reported by Gils et al. across seven countries [12], 96.4% in Tanzania [10], and 91.3% in Zimbabwe [9]. This high sensitivity is particularly critical given the clinical consequences of a missed AHD diagnosis: a false negative leaves the patient without the WHO-AHD care package, directly exposing them to fatal opportunistic infections, including cryptococcal meningitis (an estimated 223,100 annual deaths in sub-Saharan Africa) and Pneumocystis jirovecii pneumonia [15]. The 99.4% NPV confirms that a negative VISITECT result reliably excludes AHD for clinical decision-making, enabling clinicians to rule out AHD at the point of care with very high confidence.
Specificity of 89.9% is lower than in some prior evaluations but remains clinically acceptable in an AHD screening context, where a false positive triggers over-referral for confirmatory conventional CD4 testing rather than direct clinical harm. The 20 false positives (all with conventional CD4 in the near-threshold range 215-328 cells/mm3) are biologically plausible near-threshold misclassifications rather than gross errors. The concentration of 12 false positives at Homa Bay CTRH warrants investigation; temperature, humidity, lighting conditions, and specific lot quality are candidate explanations not captured by the study protocol. This site-level specificity variation has also been noted in the Gils et al. multi-country evaluation, which reported specificity ranging from 88% to 98% across sites, and attributed inter-site variation primarily to training quality and result reading conditions [12].
The near-perfect inter-reader agreement between laboratory technologists and clinicians (kappa=0.938) is the most operationally significant finding for Kenya's deployment strategy. It directly validates the task-shifting premise: that non-laboratory clinical cadres can independently interpret VISITECT results in routine practice without specialist laboratory oversight. For Kenya, where clinical officers constitute most HIV care providers at the primary healthcare facility level, dispensaries and health centres that serve the highest concentration of newly enrolled patients and IIT returnees, the exact population subgroups with the highest AHD burden, this finding unlocks the deployment model that NASCOP's hybrid CD4 strategy requires. The Luchters et al. (2019) Kenya evaluation similarly reported high concordance in a supervised setting [16], but the current study demonstrates reproducibility under routine, unsupervised, multi-site conditions, substantially strengthening the evidence base.
The finding that AHD occurred exclusively among virally unsuppressed participants (62.1% prevalence vs 0% among suppressed; chi-square=122.77, p<0.001) is a novel and clinically actionable result. This complete separation was not explained by eligibility category or clinical staging: AHD was distributed across newly enrolled (39.6%), IIT returnees (51.9%), and treatment failure (29.0%) patients, all of whom had unsuppressed viral loads. The biological plausibility is clear; virological non-suppression indicates ongoing HIV replication, progressive CD4 depletion, and accumulating immunosuppression. The programmatic implication is equally clear: VISITECT CD4 LFA deployment can be most efficiently targeted to patients presenting with confirmed unsuppressed viral loads, enabling a precision screening approach rather than universal CD4 testing of all ART-eligible patients. This would substantially reduce the number of tests required per AHD case identified, optimizing the cost-effectiveness of the 78,000-unit global fund cycle 7 allocation.
Male sex (aOR 2.40) and IIT returning to care (aOR 1.88) as independent AHD predictors are consistent with established patterns in the Kenya HIV programme. Males are systematically less engaged in HIV testing and treatment services, tend to present later in disease progression, and have lower ART adherence rates than females [5]. IIT returnees re-engage in care after periods of interrupted ART during which immune reconstitution stalls or reverses. Both groups are identifiable at clinic registration and should trigger VISITECT testing as a priority action. Kiambu County's higher AHD risk (aOR 4.63 vs Homa Bay) likely reflects the higher proportion of treatment failure and IIT patients enrolled at Thika Level 5, rather than inherently different disease biology. Note that well-controlled virally suppressed patients on stable antiretroviral therapy are managed through community-based differentiated service delivery models in Kenya and do not routinely present to facility-based HIV clinics for CD4 assessment; this reflects the NASCOP eligibility criteria that restrict CD4 testing to newly enrolled patients and those with unsuppressed viral loads.
Strengths and limitations: strengths include the real-world, multi-site, multi-county design consistent with frameworks for evaluating point-of-care diagnostics in routine low- and middle-income countries (LMIC) programmes [17]; structured evaluation of operational feasibility informed by an established implementation-science framework [18]; dual-reader performance evaluation that directly addresses task-shifting validity; large sample (n=326) exceeding the pre-specified minimum; and parallel conventional CD4 testing enabling true reference standard comparison. Limitations include the cross-sectional design, which precludes assessment of VISITECT performance longitudinally as test lots change or as operators' initial training effect fades. The Mama Lucy Kibaki Hospital specificity finding could not be fully investigated within the study scope; a dedicated site-level quality assurance investigation is warranted. Performance generalisation to community health worker settings, where pre-analytical conditions may differ further from those in structured clinic environments, requires separate evaluation. All facilities in this evaluation were level 4 and above; performance at dispensaries, health centres, and community health worker settings, where temperature, lighting, and operator training may differ substantially, requires separate prospective evaluation before routine deployment at these levels can be recommended.
VISITECT CD4 LFA confirms high operational performance in routine Kenyan public health facilities: near-perfect sensitivity (99.2%), clinically acceptable specificity (89.9%), and near-perfect inter-reader reproducibility across cadres (kappa=0.938). The actual AHD burden of 39.3% substantially exceeds current national estimates, demonstrating that the need for urgent programmatic action is greater than previously recognized. Facility-specific specificity variation (kappa 0.763-0.966) confirms that national rollouts must include site-level quality assurance protocols. NASCOP should formalize VISITECT CD4 LFA within Kenya´s national AHD diagnostic algorithm, prioritize deployment at facilities serving virally unsuppressed patients, among whom all AHD cases in this study occurred, and establish site-level quality assurance frameworks to address the operational variation identified at Mama Lucy Kibaki Hospital.
What is known about this topic
- VISITECT CD4 LFA achieves pooled diagnostic sensitivity of 91-97% in multi-country evaluations but no Kenya-specific routine-programme performance data were available prior to this study;
- Inter-reader agreement between different healthcare cadres for point-of-care diagnostic interpretation is a critical determinant of task-shifting validity but had not been evaluated for VISITECT under real-world Kenyan conditions;
- Advanced HIV disease burden among ART-eligible persons in Kenya is estimated at 32.5% nationally, but facility-level prevalence under routine programme conditions was unknown.
What this study adds
- VISITECT CD4 LFA achieves near-perfect sensitivity (99.2%) and near-perfect cross-cadre inter-reader agreement (kappa=0.938) under routine programme conditions in Kenyan public facilities, validating task-shifting to clinical officers and nurses;
- Advanced HIV disease (AHD) burden was 39.3% overall and was associated exclusively with virally unsuppressed participants (AHD prevalence 62.1% vs 0% among suppressed; p<0.001), enabling NASCOP to design a precision VISITECT screening strategy targeting unsuppressed patients rather than universal CD4 testing;
- Facility-level specificity varied significantly (kappa 0.763-0.966), with one site (Mama Lucy Kibaki Hospital) showing lower specificity (77.8%) unexplained by participant characteristics, highlighting the need for site-level quality assurance protocols in national scale-up.
The authors declare no competing interests.
John Mungai Kuria: conceptualization, data collection, analysis, drafting and revision; Tom Marwa Machera: supervision, conceptual framework, critical intellectual revision; Kathryn Nderitu: supervision, statistical review, critical revision. All the authors read and approved the final version of this manuscript.
The authors acknowledge NASCOP, the National HIV Reference Laboratory (NHRL), Amref Health Africa ESRC, the County Governments of Homa Bay, Nairobi and Kiambu, and the 326 PLHIV who participated in this study.
Table 1: baseline demographic, clinical, and immunovirological characteristics of 326 people living with HIV enrolled in a cross-sectional VISITECT CD4 lateral flow assay diagnostic accuracy and feasibility study, stratified by advanced HIV disease (AHD) status (CD4 ≤200 cells/mm3), across four public health facilities in Homa Bay, Nairobi, and Kiambu counties, Kenya (N=326)
Table 2: multivariable logistic regression of independent predictors of advanced HIV disease (CD4 ≤200 cells/mm3) among 326 people living with HIV enrolled in a cross-sectional VISITECT CD4 lateral flow assay diagnostic accuracy and feasibility study across four public health facilities in Homa Bay, Nairobi, and Kiambu counties, Kenya (n=326)
Figure 1: diagnostic accuracy of the VISITECT CD4 lateral flow assay (sensitivity, specificity, positive and negative predictive values, overall accuracy, and Cohen's kappa x100), comparing read 1 (laboratory technologist) with read 2 (clinician), against flow cytometry as the reference standard, among 326 people living with HIV across four public health facilities in Homa Bay, Nairobi, and Kiambu counties, Kenya (n=326)
Figure 2: inter-reader concordance matrix (heatmap) comparing VISITECT CD4 lateral flow assay interpretations by read 1 (laboratory technologist) and read 2 (clinician), showing the number and percentage of the 326 participants in each agreement cell, across four public health facilities in Homa Bay, Nairobi, and Kiambu counties, Kenya (n=326)
- World Health Organization. Updated Recommendations on Service Delivery for the Treatment and Care of People Living with HIV. 2021. PubMed
- Lehman A, Ellis J, Nalintya E, Bahr NC, Loyse A, Rajasingham R. Advanced HIV disease: A review of diagnostic and prophylactic strategies. HIV Med. 2023 Aug;24(8):859-876. PubMed | Google Scholar
- Joint United Nations Programme on HIV/AIDS. 2024 global AIDS report. 2024.
- Hakim J, Musiime V, Szubert AJ, Mallewa J, Siika A, Agutu C et al. Enhanced Prophylaxis plus Antiretroviral Therapy for Advanced HIV Infection in Africa. N Engl J Med. 2017 Jul 20;377(3):233-245. PubMed | Google Scholar
- National AIDS and STI Control Programme (NASCOP), Ministry of Health (Kenya). MOH Kenya Advanced HIV Disease: A Healthcare Providers Guide for Management of HIV Associated Opportunistic Infections and Condition. 2026.
- Chihana ML, Huerga H, Van Cutsem G, Ellman T, Goemaere E, Wanjala S et al. Distribution of advanced HIV disease from three high HIV prevalence settings in Sub-Saharan Africa: a secondary analysis data from three population-based cross-sectional surveys in Eshowe (South Africa), Ndhiwa (Kenya) and Chiradzulu (Malawi). Glob Health Action. 2019;12(1):1679472. PubMed | Google Scholar
- National Syndemic Diseases Control Council (NSDCC). Kenya AIDS integration strategic framework 2025-2030. 2025.
- Stevens W, Gous N, Ford N, Scott LE. Feasibility of HIV point-of-care tests for resource-limited settings: challenges and solutions. BMC Med. 2018;16(1):173. PubMed | Google Scholar
- Ndlovu Z, Massaquoi L, Bangwen NE, Batumba JN, Bora RU, Mbuaya J et al. Diagnostic performance and usability of the VISITECT CD4 semi-quantitative test for advanced HIV disease screening. PLoS One. 2020 Apr 3;15(4):e0230453. PubMed | Google Scholar
- Haraka F, Moore A, Odinga G, Bailey R, Songoro J, Haule D et al. Accuracy, use and acceptability of the VISITECT CD4 semi-quantitative test to advance HIV disease screening in routine programmatic settings in Tanzania. Clin Epidemiol Glob Health. 2024;27:101616. Google Scholar
- World Health Organization. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy, July 2017. 2017. Google Scholar
- Gils T, Hella J, Jacobs BKM, Sossen B, Mukoka M, Muyoyeta M et al. A Prospective Evaluation of the Diagnostic Accuracy of the Point-of-Care VISITECT CD4 Advanced Disease Test in 7 Countries. J Infect Dis. 2025 Feb 4;231(1):e82-e90. PubMed | Google Scholar
- Lechiile K, Leeme TB, Tenforde MW, Bapabi M, Magwenzi J, Maithamako O et al. Laboratory Evaluation of the VISITECT Advanced Disease Semiquantitative Point-of-Care CD4 Test. J Acquir Immune Defic Syndr. 2022 Dec 15;91(5):502-507. PubMed | Google Scholar
- Ministry of Health (Kenya), National AIDS & STI Control Program (Kenya). Kenya HIV prevention and treatment guidelines, 2022 edition. 2022.
- Rajasingham R, Smith RM, Park BJ, Jarvis JN, Govender NP, Chiller TM et al. Global burden of disease of HIV-associated cryptococcal meningitis: an updated analysis. Lancet Infect Dis. 2017 Aug;17(8):873-881. PubMed | Google Scholar
- Luchters S, Technau K, Mohamed Y, Chersich MF, Agius PA, Pham MD et al. Field Performance and Diagnostic Accuracy of a Low-Cost Instrument-Free Point-of-Care CD4 Test (Visitect CD4) Performed by Different Health Worker Cadres among Pregnant Women. J Clin Microbiol. 2019 Jan 30;57(2):e01277-18. PubMed | Google Scholar
- Pai NP, Vadnais C, Denkinger C, Engel N, Pai M. Point-of-care testing for infectious diseases: diversity, complexity, and barriers in low- and middle-income countries. PLoS Med. 2012;9(9):e1001306. PubMed | Google Scholar
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009 Aug 7;4:50. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PHCP






