Factors associated with essential newborn care: implications from a household survey in Lake Zone, Tanzania
Mary Drake, Jelle Stekelenburg, Regien Biesma, Young Mi Kim, Felix Bundala, Ignatus Mosten, Ruth Lemwayi
Corresponding author: Mary Drake, Department of Health Science, Global Health, University Medical Center Groningen, Groningen, Netherlands 
Received: 02 May 2025 - Accepted: 07 Apr 2026 - Published: 30 Apr 2026
Domain: Neonatology,Global health,Maternal and child health
Keywords: Infant, newborn, delivery of health care, cross-sectional studies
Funding: This work was supported by USAID and the Maternal and Child Survival Program. MOMENTUM Country and Global Leadership contributed the article processing fees for this publication through the United States Government under the terms of the Cooperative Agreement [#7200AA20CA00002], led by Jhpiego and partners. The funding body had no role in this manuscript's intellectual content and writing.
©Mary Drake et al. Primary Health Care Practice Journal (ISSN: 3105-7624). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Mary Drake et al. Factors associated with essential newborn care: implications from a household survey in Lake Zone, Tanzania. Primary Health Care Practice Journal. 2026;4:7. [doi: 10.11604/PHCP.2026.4.7.47832]
Available online at: https://www.phcp-journal.org//content/article/4/7/full
Research 

Factors associated with essential newborn care: implications from a household survey in Lake Zone, Tanzania
Factors associated with essential newborn care: implications from a household survey in Lake Zone, Tanzania
![]() Mary Drake1,2,&, Jelle Stekelenburg1, Regien Biesma1, Young Mi Kim1,3, Felix Bundala4, Ignatus Mosten5, Ruth Lemwayi5
Mary Drake1,2,&, Jelle Stekelenburg1, Regien Biesma1, Young Mi Kim1,3, Felix Bundala4, Ignatus Mosten5, Ruth Lemwayi5
&Corresponding author
Introduction: Tanzania´s newborn mortality rate is high. Like other countries, the drivers of newborn mortality in Tanzania include sepsis, prematurity/low birthweight, and complications during the intrapartum period. To help drive down newborn mortality, the World Health Organization (WHO) recommends thermal care (TC), early initiation of breastfeeding (EIBF), and clean cord care (CCC), irrespective of place of birth. This manuscript explores associations between essential newborn care (ENC) coverage and 1) the number of antenatal care (ANC) visits, 2) ANC counselling on newborn care, and 3) the place of childbirth.
Methods: data are from a population-based cross-sectional survey of recently delivered women in the Lake Zone of Tanzania. Questions were adapted from the Demographic and Health Survey and the United States Agency for International Development Child Survival and Health Grants Program. Bivariate and multivariate logistic regression analyses were conducted to examine associations between essential newborn care (ENC), TC, EIBF, CCC, and predictors.
Results: coverage of ENC was suboptimal, with 30.8% of newborns receiving TC, 73.6% getting EIBF, and 46.8% receiving CCC. The odds of TC were higher at facility births as compared to home births (aOR 5.63; CI 3.89-8.14). EIBF had increased odds with ANC counselling on newborn care (aOR 2.35; CI 1.78-3.11). Odds of CCC were lower among facility births compared to home births (aOR 0.54; CI 0.42-0.69).
Conclusion: strengthening ANC counselling is critical to enhancing awareness of TC. Building the capacity of providers working in postnatal wards may improve CCC. A more comprehensive approach integrating facility-based and community-level interventions may help ensure equitable access to ENC practices. Expanding coverage and improving the quality of ENC interventions will contribute to improved newborn health outcomes across different birth settings.

The newborn period is extremely vulnerable and has the highest risk for mortality of all the periods of childhood [1]. It is estimated that in 2022, there were 4.9 million deaths of children under the age of 5, and 47% of these (2.3 million) occurred in children in the first 28 days of life, with a large proportion in sub-Saharan Africa [1]. With ambitious Sustainable Development Goals (SDG) for newborn mortality to reach 12 per 1,000 live births globally, and a large proportion of newborn deaths being preventable [2], coverage of evidence-based interventions is critical. In Tanzania, the current newborn mortality rate (NMR) is 24/1,000 live births and has been reduced only marginally in the last ten years [3]. Like many countries, the drivers of newborn mortality in Tanzania include sepsis, prematurity/low birthweight, and complications during the intrapartum period. For a strong foundation for all babies, the World Health Organization (WHO) recommends, among other interventions, thermal care, early initiation of breastfeeding within one hour of birth (EIBF), and clean umbilical cord care [4,5].
Thermal care (skin-to-skin, delayed bathing, and a head covering) protects newborns from hypothermia and can help avert up to 10% of full-term newborns and 20% of preterm newborn mortality [6]. Estimates show that EIBF saves lives across all causes of newborn mortality [7]. Clean cord care averts deaths due to omphalitis-related neonatal sepsis and neonatal tetanus. While earlier studies in Bangladesh, Nepal, Pakistan, and India showed chlorhexidine (CHX) to reduce newborn mortality [8,9], later studies from Zambia [10] and Tanzania [11] showed no significant difference in mortality between CHX application and dry cord care. The WHO currently recommends not placing anything on the cord where the neonatal mortality is below 30 deaths per 1,000 live births [5].
Previous studies showed mixed results with regard to factors that influence essential newborn care, such as the number of antenatal care (ANC) visits, ANC counselling on newborn care, and place of birth. In India, Isac et al. explored facility-level factors associated with ENC and found that only 26.2% of newborns received full ENC and that the odds of ENC were higher in facilities with providers with higher levels of skills and knowledge, and wide variation between facility types [12]. Similarly, Salo et al. in Ethiopia found odds of ENC were higher among providers with ENC knowledge and who received supportive supervision, among other factors [13]. These two studies explored facility births. Other studies included facility and home births. Aboagye et al. [14], Teshale et al. [15] and Appiah et al. [16] analyzed demographic and health survey (DHS) data from sub-Saharan African countries and found that EIBF was associated with facility childbirth or those assisted by skilled attendants. Appiah found EIBF was also associated with having 4 or more ANC visits [16].
Regional studies further illustrate variations in ENC by birthplace. In Peru, Reinders et al. found ENC was lower in home births as compared to facility births [17]. Similarly, in India, Devasenapathy et al. showed a strong association between facility births and ENC [18]. In contrast, Olorunsaiye et al. in Benin [19] and Waiswa et al. in Uganda [20] found no association between ENC and birth location.
Findings on ANC counselling and ENC are also mixed. Two studies in Ethiopia showed a positive association between getting information on ENC during ANC and ENC practice [21,22]. Conversely, findings from Uganda indicated no association between ANC and ENC [20].
Given these mixed results on the associations between place of childbirth, ANC counselling, and ENC coverage, this study aims to examine associations between ENC coverage and 1) the number of ANC visits, 2) ANC counselling on newborn care, and 3) the place of childbirth. Understanding these associations will help inform interventions aimed at increasing ENC coverage and improving neonatal health outcomes in Tanzania and similar contexts.

Survey design and setting: this study analyzes data from a cross-sectional household survey conducted by the USAID-funded Maternal Child Survival Program (MCSP) in April 2016 in the Mara and Kagera regions of Tanzania. The Maternal Child Survival Program (MCSP) was a reproductive, maternal, newborn, and child health project in these two regions. These two regions were selected in collaboration with the Government of Tanzania because they were considered to be contributing heavily to maternal and newborn mortality [23]. The survey explored knowledge, practices, and coverage (KPC) in the areas of maternal and newborn health, immunization, malaria, and family planning. Data presented in this paper focus on a subset of the KPC maternal and newborn survey data.
Sampling and sample size: a two-stage stratified cluster sampling method was used for the KPC survey. Mara and Kagera, the MCSP program implementation regions, are administratively organized into districts and then wards, each with rural and urban areas. The Tanzania HIV/AIDS and Malaria Indicator Survey and the 2012 population census wards were further broken down into enumeration areas (EA). Each EA demarcated a smaller boundary assigned to avoid overlap between villages and included approximately 100 households.
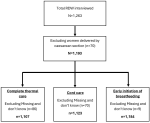
In the KPC survey, 64 EAs were randomly selected (32 from each region) using the probability proportional to size (PPS) method within each urban and rural geographical strata, based on household size data from the recent census (2012). At each EA, a household list was used to systematically select 20 households (fixed take-size) which had women aged 15-49 years old who had delivered in the past two years (termed recently delivered women (RDW)). Households were visited in sequence as they appeared in the list to locate potential survey participants. At the household level, survey staff listed all RDW and solicited informed consent. If there was more than one eligible participant in a household, all of them were included in the sample. A total of 1,263 women were interviewed (Kagera=629; Mara=634). Of these, 70 women who gave birth by caesarean section were excluded from this analysis because the recall of the women would be affected by general anesthesia (the mode of anesthesia for C-section in Tanzania), resulting in a final sample of 1,193 women (Kagera=586; Mara=607). Additional details on the specific sample included in each analysis are included in Figure 1.
Data collection: interviews were conducted using the KPC survey structured questionnaires developed by the Maternal and Child Survival Program. The questionnaires were adapted and translated from English to Kiswahili and pretested to ensure comprehension, local context appropriateness, and fit into the Tanzanian context. The questionnaires were uploaded into tablets in the CommCare HQ mobile data collection platform. A team of 30 research assistants (male and female) was trained for four days on research ethics (obtaining informed consent, respecting voluntary participation of respondents, privacy, and confidentiality of data collected), sampling and household selection, survey administration, and data management. Face-to-face interviews using the Kiswahili language were conducted. Data quality was ensured by built-in skip patterns in the questionnaire. Additionally, a data manager reviewed the study database on a daily basis to assess the completeness of data and alerted survey supervisors to errors so that they could be addressed immediately. The tablets used for data collection were password-protected to ensure the confidentiality of collected data. The study database was stored on a server and accessible by password to the study team only.
Data analysis
Variables
Dependent variables (outcomes): the outcome variables include thermal care, clean cord care, and EIBF. Thermal care is a composite indicator defined as: 1) newborn was dried/wrapped before the placenta or immediately after the placenta was delivered or within 1 hour after delivery; 2) baby was placed skin to skin with the mother within 1 hour after delivery; and 3) bathing of the baby was delayed 24 hours or more after birth. Clean cord care was defined as nothing applied to the umbilical cord after the cord was cut and tied until the cord fell off. EIBF was defined as breastfed within 1 hour of birth.
Independent variables: the independent variables were drawn from previously published literature on newborn health and include predisposing and enabling factors. Primary exposures of interest were the place of childbirth, the number of ANC visits attended, and ANC counselling on newborn care. The place of the woman´s most recent childbirth was categorized as home or health facility, whereby home included their own home or that of someone else, or with a traditional birth attendant. The number of ANC visits attended during pregnancy was grouped into: a) no ANC visit; b) one to three visits; and c) at least four visits. ANC counselling on newborn care was defined as the mother receiving any counselling on either danger signs for the newborn, initiation of breastfeeding, or exclusive breastfeeding. Sociodemographic characteristic variables included in the analysis were age, mother´s education, marital status, and socioeconomic status.
Statistical analysis: the data were cleaned, coded, and analyzed using Stata 15. Clustering at the sub-village/hamlet was adjusted using Huber-White standard errors. Frequencies and percentages were used to summarize the data. Crude odds ratios (OR) with 95% confidence intervals were estimated with binary logistic regression analysis to assess the magnitude of association between each independent variable and the outcome variables, and inclusion of variables for the multivariable logistic regression analysis. Variables with p-value < 0.2 in the unadjusted binary logistic regression analysis were considered in the multivariable logistic analysis. The Hosmer-Lemeshow goodness-of-fit test with the enter procedure was used to test for model fitness. An adjusted odds ratio with 95% confidence interval was estimated to assess the strength and direction of the association. In this study, multi-collinearity among independent variables (parity and mother´s age) was checked using the variance inflation factor (VIF) on regression analysis. Variables with p-value < 0.05 in the multivariable logistic regression analysis were considered as significant and independent predictors.
Ethical considerations: this survey was reviewed and received ethical approval from the Johns Hopkins School of Public Health Institutional Review Board (IRB) (IRB# 00005931) and the Medical Research Coordinating Committee (MRCC) of the National Institute for Medical Research (NIMR) of Tanzania (IRB# NIMR/HQ/R.8a.Vol. IX/2131). A consent script in the Kiswahili language was read to the participant by the research assistant, and the participant was given an opportunity to ask questions, which were answered by the research assistant before consenting. When a participant agreed to participate, an identification number was provided, and documentation of consenting was done by the research assistant signing the written consent form. For women aged 15-17 years who had a child but were not married, parental/guardian permission was required in addition to the woman´s own consent for enrollment in the survey. Interviews were conducted by data collectors in the homestead of the participant in an area that provided privacy and where no one could overhear the conversation between the interviewee and interviewer.
Of all the women interviewed, about half (573 women) were below age 25. The majority (70%) had a primary level of education; 87.9% were married; 20% had a middle household wealth index, while 40% each had low and high index. Health service utilization characteristics included that 65.5% gave birth in a health facility, 52.1% had 4 or more ANC visits, and 58.4% received ANC counselling on newborn care (Table 1). Of respondents interviewed, 74% reported EIBF, just under half (47%) reported clean cord care, and 30% reported complete thermal care. A mere 9.6% received all (Table 2).
Place of childbirth. In bivariate analysis, odds of thermal care were significantly higher among births at health facilities as compared to births at home (OR 6.25, p<0.001). In contrast, the odds of the newborn receiving cord care were significantly lower among births at health facilities as compared to births at home (OR 0.52, p<0.001). These remained significant in the multivariate analysis (Table 3). The odds of EIBF were not significantly different between facility and home deliveries.
Antenatal care counselling on newborn care. In bivariate analysis, the odds of EIBF were significantly higher when ANC counselling included content on newborn care (OR 2.42, p<0.001). This remained significant in multivariate analysis (Table 3). ANC counselling on newborn care was not associated with thermal care or cord care. Number of ANC visits. The number of ANC visits was not a significant predictor of any of the components of ENC (Table 4, Table 5, Table 6).
This study explored factors associated with ENC (EIBF, thermal care, and clean cord care). Our findings indicate that place of birth and antenatal care counselling on newborn care are associated with ENC. Regarding place of childbirth, number of ANC visits, and ANC counselling on newborn care, our study found that thermal and clean cord care are associated with HF birth, with higher odds of thermal care and lower odds of clean cord care, among facility births. Neither thermal care nor clean cord care was associated with the number of ANC visits or ANC counselling on NB care. In contrast, EIBF was associated with ANC counselling on NB care but not with the number of ANC visits nor place of childbirth. Despite policies promoting essential newborn care (ENC) through skilled birth attendance and antenatal care (ANC) programs [24,25], our findings reveal that birthing at a facility does not guarantee that newborns will receive the required care. This aligns with studies from Tanzania [14,15,26-28], Kenya [29], Benin [19], Ethiopia [26], Uganda [20] and Peru [17]. The overall low coverage of ENC is concerning, especially as these interventions do not require advanced technology and have the potential to reach all births. Although the facility is the optimal place for birth as the setting is designed to manage not only ENC but also emergency situations, some births still take place in communities or on the way to the facility, for various reasons.
Our study found an EIBF rate of 74%, which is higher than previous estimates from Tanzania that reported a 52% rate [14-16]. Reasons for our study results being different may be that they are from a survey in Tanzania from a later period, and that the survey was powered for two regions. Similar rates of EIBF to our study were found in Peru [17]. Our findings align with previous studies [14,15,18,20] in showing no association between EIBF and number of ANC visits. This contrasts with Appiah et al. study [16] who found a small association with the number of visits. A possible explanation is that ANC contact is not a good measure because it falls short of measuring what was done during the visit, consistent with Benova et al. [30]. However, our study found that specific counselling on newborn care during ANC was associated with EIBF, similar to findings from Ethiopia [22]. One explanation for this finding may be that, compared to other elements of ENC, EIBF requires active participation of the mother, and therefore, counselling highly influences the application of the practice. On the other hand, a contribution may also come from the fact that the current ANC guidelines include EIBF. In Tanzania, attendance for ANC at least once is universal [3], therefore can serve as an anchor for counselling and educating the mother on all elements of ENC.
Unlike Aboagye et al. Teshale et al., Appiah et al. and Devasenapathy et al. [14-16,18], our results showed no difference between community and facility births in EIBF. A reason for the difference may be that breastfeeding has been promoted consistently in Tanzania, not only in ANC but across various health sector interventions as a component of nutrition through different media, reaching policy makers, program implementers, and the public.
Thermal care was low for all births. Among the three elements of thermal care studied, immediate drying was highest, followed by delayed bathing and then skin-to-skin (STS) care. Similar to our study, low STS has been documented in other studies from Tanzania [26-28,31,32], Kenya [29], Ethiopia [33], Ghana, Malawi, Zambia and Uganda [26]. Despite being low, the odds of a newborn getting thermal care were higher for births at the facility level. Our finding is similar to findings from Mallick et al. in India, Nepal, and Bangladesh, which found higher odds of thermal care when birth was with a skilled birth attendant [34]. A study out of Kenya [29] further found that delayed bathing was not associated with poor thermal care, and findings from Shamba et al. indicate that healthcare worker advice is a reason women delay bathing the newborn [31]. Wako et al. in Ethiopia found that newborns were bathed in the first six hours after birth [33]. In Tanzania, the policy indicates that all women giving birth at a facility should stay for at least 24 hours, and being in the facility may prevent mothers from bathing babies early.
Clean cord care was around 47% in our sample. Results of a large community-based study in Southern Tanzania showed that only 28% of newborns had something put on the cord [27]. Possible reasons for the difference may be the time period that the study took place and that our study area, the Lake Zone, tends to have worse newborn health indicators as compared to southern Tanzania [23]. Newborns of women who gave birth at home had higher odds of clean cord care compared to those delivered at the facility. These findings are consistent with results from a systematic review by Coffey et al. which showed that in Tanzania, dry cord care has reached all levels of society [35]. It is also possible, however, that women birthing in facilities reported that something was put on the cord out of courtesy bias, feeling that something should have been put on the cord for facility births.
Strengths and limitations: this is a population-based, representative survey among RDW in the Lake Zone, Tanzania, an area of the country seen as driving up maternal mortality. Understanding what is happening there at a population level is very important. Many of the questions used were from the Demographic and Health Survey, so they were not created uniquely for this study. The data do not report out on observations, thus can be affected by recall bias. The cord care question could also be affected by courtesy bias, and women who had a facility birth may have answered the question of whether anything was put on the cord as �yes� because they thought that was the expected answer. Despite being based on 2016 data, our study contributes valuable insights into factors associated with ENC and can serve as a benchmark to which newer studies can track trends over time.
Future research: rigorous study of quality improvement efforts to improve ENC, similar to the work of Jain et al. in India [36], can drive deeper understanding of what works and strengthen implementation of these effective interventions. Community-based education [37] has been shown to be effective and should be implemented, and ENC outcomes should be assessed. Future studies can contribute to the evidence by rigorously assessing the quality of newborn counselling in ANC, exploring shifts in agency of the mother and her intention to deliver at a facility, and engaging in optimal ENC practices. Additionally, building on the work like that of Salo et al. [13] and Isac et al. [12], future studies can explore provider and facility-related factors associated with ENC practices.
Our study supports findings from other studies, reinforcing the importance of structured ANC education promoting optimal breastfeeding practices, and also highlights some differences that add to the evidence base in Tanzania and globally. Strengthening ENC at both facility and community levels is essential, using an integrated continuum-of-care approach. Being low-tech, the interventions are feasible to implement in both settings, and existing experiences should be leveraged for improving community education, service quality, and health outcomes. Furthermore, these findings call for updating the ANC counselling package to include all elements of ENC, particularly thermal care, as well as to improve the quality of ANC counselling. Tanzania is well-positioned to implement these within the current policy environment and commitment to strengthen maternal and newborn health laid out in One Plan III and HSSP V.
What is known about this topic
- Newborn mortality is stagnating, and the need to reduce it is urgent;
- Essential newborn care (ENC) can help improve neonatal survival and provide a strong foundation for infant development;
- There are mixed results regarding factors associated with ENC outcomes.
What this study adds
- There are higher odds of thermal care among health facility births as compared to home births;
- The odds of EIBF are higher when ANC counselling on newborn care is provided as compared to when it is not;
- Odds of clean cord care are higher among home births as compared to facility births.
The authors declare no competing interests.
Mary Drake: conceptualization and drafted the manuscript; Jelle Stekelenburg and Felix Bundala: critical review; Young Mi Kim: conceptualization and critical review; Regien Biesma: conceptualization, critical review, and editing; Ruth Lemwayi: drafted methods section and critical review; Ignatus Mosten: participated in drafting introduction and discussion, critical review. All the authors read and approved the final version of this manuscript.
We wish to acknowledge the women and communities in Mara and Kagera for their time and effort participating in the study; to the district and regional health teams, the national Ministry of Health Reproductive and Child Health Services unit; Dr. Diwakar Mohan of JHU, the enumerators and Jhpiego staff involved in the planning and implementation of the household survey.
Table 1: sociodemographic and health use characteristics of recently delivered women participating in the household survey in Lake Zone, Tanzania (N=1,263)
Table 2: thermal care, cord care, and immediate breastfeeding by socio-demographic characteristics and health service use of recently delivered women participating in the household survey in Lake Zone, Tanzania
Table 3: multivariate logistic regression analysis of thermal care, cord care, breastfeeding within one hour, essential newborn care (ENC), and place of birth, antenatal care visit, and antenatal care counselling among recently delivered women participating in the household survey in Lake Zone, Tanzania
Table 4: bivariate analysis of thermal care (outcome) and explanatory variables based on a household survey of recently delivered women in Lake Zone, Tanzania
Table 5: bivariate analysis of early initiation of breastfeeding (outcome) and explanatory variables based on a household survey of recently delivered women in Lake Zone, Tanzania
Table 6: bivariate analysis of cord care (outcome) and explanatory variables based on a household survey of recently delivered women in Lake Zone, Tanzania
Figure 1: schematic presentation of the number of recently delivered women in the survey, inclusions, and exclusions during analysis
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Levels & Trends in Child Mortality: Report 2023, Estimates developed by the United Nations Inter-agency Group for Child Mortality Estimation, United Nations Children�s Fund, New York. 2024. Accessed 29th April, 2025.
- Lawn JE, Bhutta ZA, Ezeaka C, Saugstad O. Ending Preventable Neonatal Deaths: Multicountry Evidence to Inform Accelerated Progress to the Sustainable Development Goal by 2030. Neonatology. 2023;120(4):491-499. PubMed | Google Scholar
- Ministry of Health (MoH) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2022. 2022. Accessed 12th December, 2024.
- World Health Organization. WHO recommendations: intrapartum care for a positive childbirth experience. 2018.
- World Health Organization. WHO recommendations on maternal and newborn care for a positive postnatal experience. 2022. PubMed | Google Scholar
- Bhutta ZA, Das JK, Bahl R, Lawn JE, Salam RA, Paul VK et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. 2014 Jul 26;384(9940):347-70. PubMed | Google Scholar
- NEOVITA Study Group. Timing of initiation, patterns of breastfeeding, and infant survival: prospective analysis of pooled data from three randomised trials. Lancet Glob Health. 2016 Apr;4(4):e266-75. PubMed | Google Scholar
- Shariff JA, Lee KC, Leyton A, Abdalal S. Neonatal mortality and topical application of chlorhexidine on umbilical cord stump: a meta-analysis of randomized control trials. Public Health. 2016 Oct;139:27-35. PubMed | Google Scholar
- Imdad A, Mullany LC, Baqui AH, El Arifeen S, Tielsch JM, Khatry SK et al. The effect of umbilical cord cleansing with chlorhexidine on omphalitis and neonatal mortality in community settings in developing countries: a meta-analysis. BMC Public Health. 2013;13 Suppl 3(Suppl 3):S15. PubMed | Google Scholar
- Semrau KEA, Herlihy J, Grogan C, Musokotwane K, Yeboah-Antwi K, Mbewe R et al. Effectiveness of 4% chlorhexidine umbilical cord care on neonatal mortality in Southern Province, Zambia (ZamCAT): a cluster-randomised controlled trial. Lancet Glob Health. 2016 Nov;4(11):e827-e836. PubMed | Google Scholar
- Sazawal S, Dhingra U, Ali SM, Dutta A, Deb S, Ame SM et al. Efficacy of chlorhexidine application to umbilical cord on neonatal mortality in Pemba, Tanzania: a community-based randomised controlled trial. Lancet Glob Health. 2016 Nov;4(11):e837-e844. PubMed | Google Scholar
- Isac S, Dehury B, Prakash R, Hasan N, Anthony J, Ramesh BM et al. Essential newborn care practices in selected public health facilities using observation of 2603 normal deliveries in Uttar Pradesh, India. BMJ Glob Health. 2025 Jan 31;10(1):e017117. PubMed | Google Scholar
- Salo SS, Ukumo EY, Teshale MY. Factors associated with essential newborn care practice among obstetric care providers in public hospitals in Gamo, Gofa, and Wolayta zones, southern Ethiopia: A facility-based cross-sectional study, 2022. PLoS One. 2024 Dec 27;19(12):e0314767. PubMed | Google Scholar
- Aboagye RG, Ahinkorah BO, Seidu AA, Anin SK, Frimpong JB, Hagan JE Jr. Mother and newborn skin-to-skin contact and timely initiation of breastfeeding in sub-Saharan Africa. PLoS One. 2023 Jan 10;18(1):e0280053. PubMed | Google Scholar
- Teshale AB, Tesema GA. Timely initiation of breastfeeding and associated factors among mothers having children less than two years of age in sub-Saharan Africa: A multilevel analysis using recent Demographic and Health Surveys data. PLoS One. 2021 Mar 23;16(3):e0248976. PubMed | Google Scholar
- Appiah F, Ahinkorah BO, Budu E, Oduro JK, Sambah F, Baatiema L et al. Maternal and child factors associated with timely initiation of breastfeeding in sub-Saharan Africa. Int Breastfeed J. 2021 Jul 19;16(1):55. PubMed | Google Scholar
- Reinders S, Blas MM, Neuman M, Huicho L, Ronsmans C. Prevalence of essential newborn care in home and facility births in the Peruvian Amazon: analysis of census data from programme evaluation in three remote districts of the Loreto region. Lancet Reg Health Am. 2022 Dec 5;18:100404. PubMed | Google Scholar
- Devasenapathy N, Neogi SB, Soundararajan S, Ahmad D, Hazra A, Ahmad J et al. Association of antenatal care and place of delivery with newborn care practices: evidence from a cross-sectional survey in rural Uttar Pradesh, India. J Health Popul Nutr. 2017 Jun 21;36(1):30. PubMed | Google Scholar
- Olorunsaiye CZ, Yusuf KK, Harris AM, Gaikwad S. Essential newborn care practices in Benin: Are there differences by birth location? Birth. 2021 Dec;48(4):514-523. PubMed | Google Scholar
- Waiswa P, Peterson S, Tomson G, Pariyo GW. Poor newborn care practices - a population based survey in eastern Uganda. BMC Pregnancy Childbirth. 2010 Feb 23;10:9. PubMed | Google Scholar
- Berhea TA, Belachew AB, Abreha GF. Knowledge and practice of Essential Newborn Care among postnatal mothers in Mekelle City, North Ethiopia: A population-based survey. PLoS One. 2018 Aug 22;13(8):e0202542. PubMed | Google Scholar
- Chichiabellu TY, Mekonnen B, Astawesegn FH, Demissie BW, Anjulo AA. Essential newborn care practices and associated factors among home delivered mothers in Damot pulasa Woreda, southern Ethiopia. Reprod Health. 2018 Sep 27;15(1):162. PubMed | Google Scholar
- Afnan-Holmes H, Magoma M, John T, Levira F, Msemo G, Armstrong CE et al. Tanzania´s Countdown to 2015: an analysis of two decades of progress and gaps for reproductive, maternal, newborn, and child health, to inform priorities for post-2015. Lancet Glob Health. 2015 Jul;3(7):e396-409. PubMed | Google Scholar
- The United Republic of Tanzania Ministry of Health, Community Development, Gender, Elderly and Children. National Plan for Reproductive, Maternal, Newborn, Child and Adolescent Health & Nutrition (2021/2022 - 2025/2026) One Plan III. 2021. Accessed 12th November, 2024.
- United Republic of Tanzania Ministry of Health, Community Development, Gender, Elderly and Children. Health Sector Strategic Plan July 2021 - June 2026 (HSSP V) Leaving No One Behind. 2021. Accessed 12th December, 2024.
- Bee M, Shiroor A, Hill Z. Neonatal care practices in sub-Saharan Africa: a systematic review of quantitative and qualitative data. J Health Popul Nutr. 2018 Apr 16;37(1):9. PubMed | Google Scholar
- Penfold S, Hill Z, Mrisho M, Manzi F, Tanner M, Mshinda H et al. A large cross-sectional community-based study of newborn care practices in southern Tanzania. PLoS One. 2010 Dec 21;5(12):e15593. PubMed | Google Scholar
- Manji K. Situation analysis of newborn health in Tanzania: Current situation, existing plans and strategic next steps for newborn health. 2009. Accessed 22nd October, 2019.
- Nyandiko WM, Kiptoon P, Lubuya FA. Neonatal hypothermia and adherence to World Health Organisation thermal care guidelines among newborns at Moi Teaching and Referral Hospital, Kenya. PLoS One. 2021 Mar 23;16(3):e0248838. PubMed | Google Scholar
- Benova L, Tunçalp Ö, Moran AC, Campbell OMR. Not just a number: examining coverage and content of antenatal care in low-income and middle-income countries. BMJ Glob Health. 2018 Apr 12;3(2):e000779. PubMed | Google Scholar
- Shamba D, Schellenberg J, Hildon ZJ, Mashasi I, Penfold S, Tanner M et al. Thermal care for newborn babies in rural southern Tanzania: a mixed-method study of barriers, facilitators and potential for behaviour change. BMC Pregnancy Childbirth. 2014 Aug 11;14:267. PubMed | Google Scholar
- Adejuyigbe EA, Bee MH, Amare Y, Omotara BA, Iganus RB, Manzi F et al. "Why not bathe the baby today?": A qualitative study of thermal care beliefs and practices in four African sites. BMC Pediatr. 2015 Oct 14;15:156. PubMed | Google Scholar
- Wako WG, Beyene BN, Wayessa ZJ, Fikrie A, Amaje E. Assessment of neonatal thermal cares: Practices and beliefs among rural women in West Guji Zone, South Ethiopia: A cross-sectional study. PLOS Glob Public Health. 2022 Jun 15;2(6):e0000568. PubMed | Google Scholar
- Mallick L, Yourkavitch J, Allen C. Trends, determinants, and newborn mortality related to thermal care and umbilical cord care practices in South Asia. BMC Pediatr. 2019 Jul 22;19(1):248. PubMed | Google Scholar
- Coffey PS, Brown SC. Umbilical cord-care practices in low- and middle-income countries: a systematic review. BMC Pregnancy Childbirth. 2017 Feb 20;17(1):68. PubMed | Google Scholar
- Jain M, Meshram P, Bang A, Chauhan V, Datta V, Dhanireddy R. Implementation of a quality improvement initiative for standardising essential newborn care in a teaching public hospital in rural central India. BMJ Open Qual. 2024 Apr 16;13(Suppl 1):e001869. PubMed | Google Scholar
- Lassi ZS, Kedzior SG, Bhutta ZA. Community-based maternal and newborn educational care packages for improving neonatal health and survival in low- and middle-income countries. Cochrane Database Syst Rev. 2019 Nov 5;2019(11):CD007647. PubMed | Google Scholar
Search

This article authors
On Pubmed
On Google Scholar
Citation [Download]
Navigate this article
Similar articles in
Key words
Tables and figures
Article metrics
Recently from the PHCP